Restorative Dentistry
Effect of contaminants and damage of the light guide tip and the use of barrier sleeves on the efficiency of the LCUs
Summary
The aim of this study is to conduct an experiment on the light curing units used in clinical and pre-clinical dental practices to perceive the possible effects of contaminants on the light guide tip of the LCUs and its degree, and the use of protective barrier sleeves to cover the light guide of the same LCUs. Additionally, we are going to assess whether LCU tip's damage such as chipping, dents and scratches can cause any energy deterioration delivered by the LCUs.
Introduction
Light curing is a crucial step in the restorative dentistry during the application of light-activated resin-based composites (RBC), however it usually does not receive the proper awareness it deserves and often taken for granted which may lead to the failure of these restorations, and with the increased demand and use of RBCs, light-cured cements, and adhesives, as well as the extensive usage of light curing units in other dental procedures, like orthodontics and bleaching, LCUs have become an essential and heavily used equipment in any dental practice, and with this expanded use of LCUs comes an issue of contamination and damage of the LCU’s light guide tip, which raises the question on the effect of such contaminants like cured RBCs remnants and other materials on the tip of the LCU on its efficiency to deliver the required energy to sufficiently cure the RBCs and to what degree. Furthermore, a damage to the light guide might occur while handling the LCU such as scratches, dents or chipping of its tip, and while it’s logical to get a damaged dental equipment replaced, some dental practices might ignore the issue and continue to use the damaged LCU.
Although several studies have suggested maintaining the LCUs and keeping them clean and free of contaminants, there is a lack of scientific evidence or data in the literature on the consequences of not doing so and to what degree it can affect the amount of energy delivered by the LCUs. Moreover, it was stated that the use of protective barriers to cover the light guide can diminish the energy delivered by the LCU by up to 10%, therefore we wanted to cover this point of interest in our study.
In light curing terminology the term irradiance is used to describe the power output of the LCU and expressed in units of (mW/cm²), which is the radiant power delivered by the LCU on a surface and shows what the resin receives. Another important term is the radiant energy which is the amount of energy received by a surface area over time (irradiance x time = energy/area = J/cm²). A further element is the recommended amount of energy to be received by the composite which has been suggested to be 8-16 J/cm². Also, it was advocated to use LCUs with light intensity (Irradiance) of not less than 300 mW/cm².
Some studies have showed that most dentists do not know the power of the LCUs they use, or the amount of energy different resin-based composites need to receive for sufficient curing and adequate polymerization, which makes them susceptible to having composite restorations that aren’t polymerized ideally. This leads us to the issue of these dentists lacking attention to maintaining and cleaning their LCUs regularly. Therefore, we aim with this study to observe the significance of care and maintenance of the LCUs to educate dental care professionals.
Materials and Methods
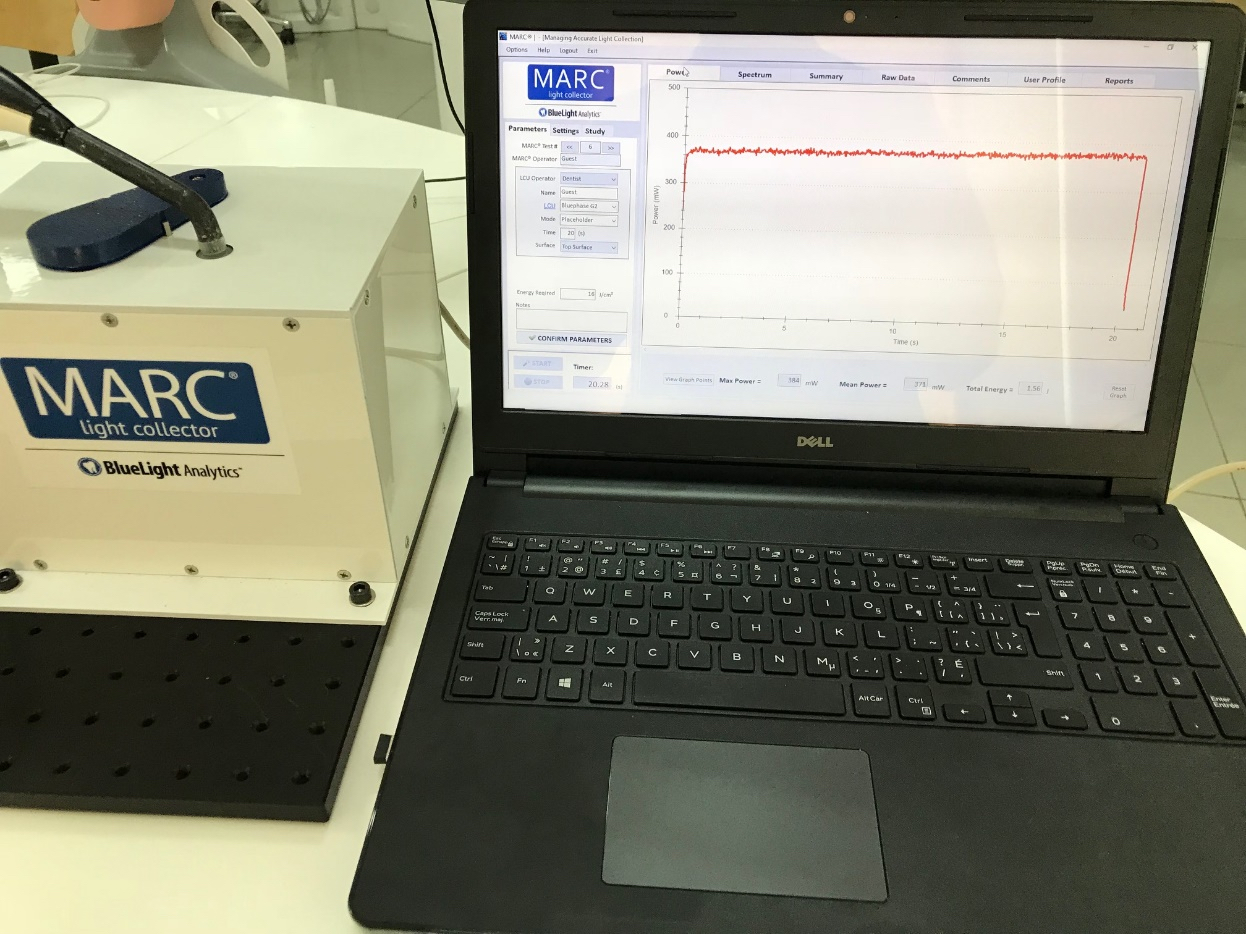
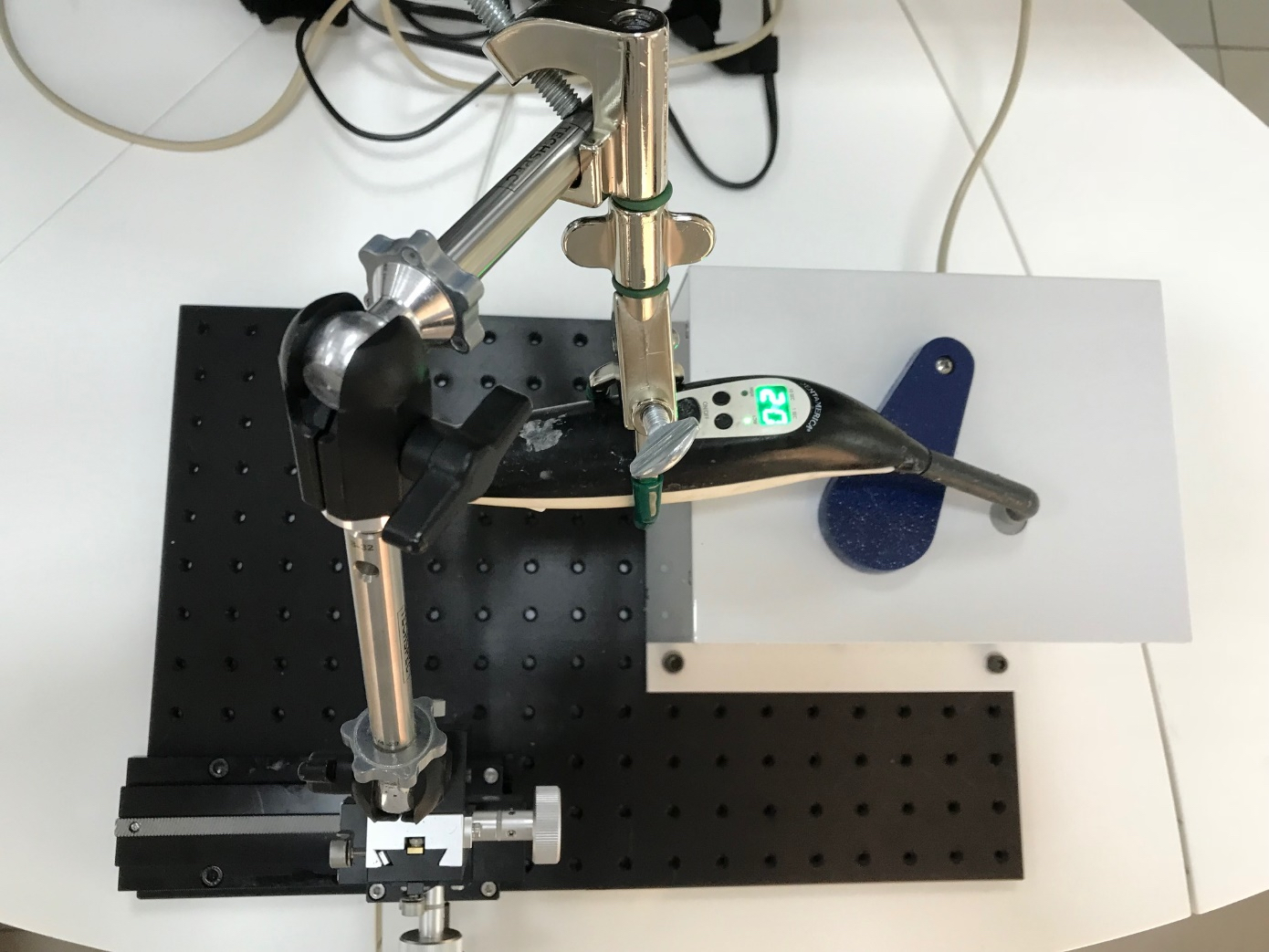
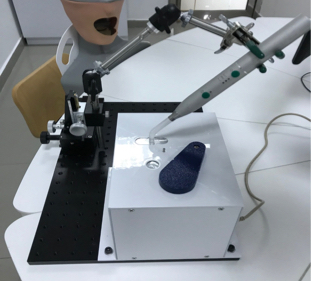
In this experiment we will use the MARC™ Light Collector by BlueLight Analytics™ which utilizes a laboratory grade spectrometer (USB 4000, Ocean Optics) to accurately record the irradiance and energy delivered to the sensors that are 3.9mm in diameter and similar to a Class I preparation, those sensors are connected to the spectrometer with a bifurcated fibre optic cable. We will measure the tip irradiance of the LCU and the total energy delivered to the top surface of the specimen at a zero distance from the tip to the specimen. A pre-configured laptop computer prepacked with the custom MARC™ software, incorporates data gathering, storage, exporting, and reporting. The MARC™ resin calibrator is fixed on a special bench in addition to a specifically designed modifiable accessory arms that allows the LCU to be fixed accurately into the desired position over the sensors and moved without readjusting the height. This enables the calibration of the LCUs over the sensors, so we can assure that every LCU is positioned exactly the same every time we run the test. Furthermore, an LCU that was used for the calibration of the device prior to the study will be used between tests to guarantee that the device is giving accurate measurements.
Four main stages of testing the LCUs are included: initially, each LCU will be tested after taking them from the clinics and the pre-clinical labs in Ajman University without informing the responsible staff about cleaning or maintaining these LCUs to accurately measure the power output and energy delivered by these units with contaminants and debris present on the light guide tip. The next stage is to put a barrier sleeve on these LCUs and test their power, while the following stage is to remove the barrier, clean the light guide with proper cleaning methods to ensure that it’s free from any debris and to get the tip as clear as possible before running the test again. On the final stage, we get the barrier sleeve on the cleaned LCU and run the test.
On a separate secondary experiment, we are going to test some LCUs with damaged tip and replace this tip with a new one and test it again to see to what degree the damage can affect the power output of the LCUs.
The MARC™ Light Collector software by BlueLight Analytics™ will be used to run the tests and collect real time data from the resin calibrator and save them, this software can display several points of interest such as mean irradiance, max irradiance, total energy, wavelength and time required to deliver the energy needed to cure the RBCs.
A total of 25 LCUs will be collected, each will go through the four stages of testing, an additional two or three LCUs with damaged light guide tip will go through the secondary test. All the data will be collected and exported for statistical analysis which will be achieved using the IBM SPSS Software to compare between the sample groups.
Below are some pictures showing the equipments and the preparations for the project.
Effect of angulation of light curing units on the polymerization of resin-based composites
The purpose of this study is to carry out an experiment on the effect of angulation of the light curing units on the polymerization of resin-based composites. The method we will use is to measure the degree of conversion (DC) that occurs during the curing process and even hours post-curing which will show how different angulations of the light guide tip to the resins can lead to different quality of polymerization of the composites. Therefore, we can recognize the importance of angulation of the LCUs which is frequently overlooked during regular dental practice.
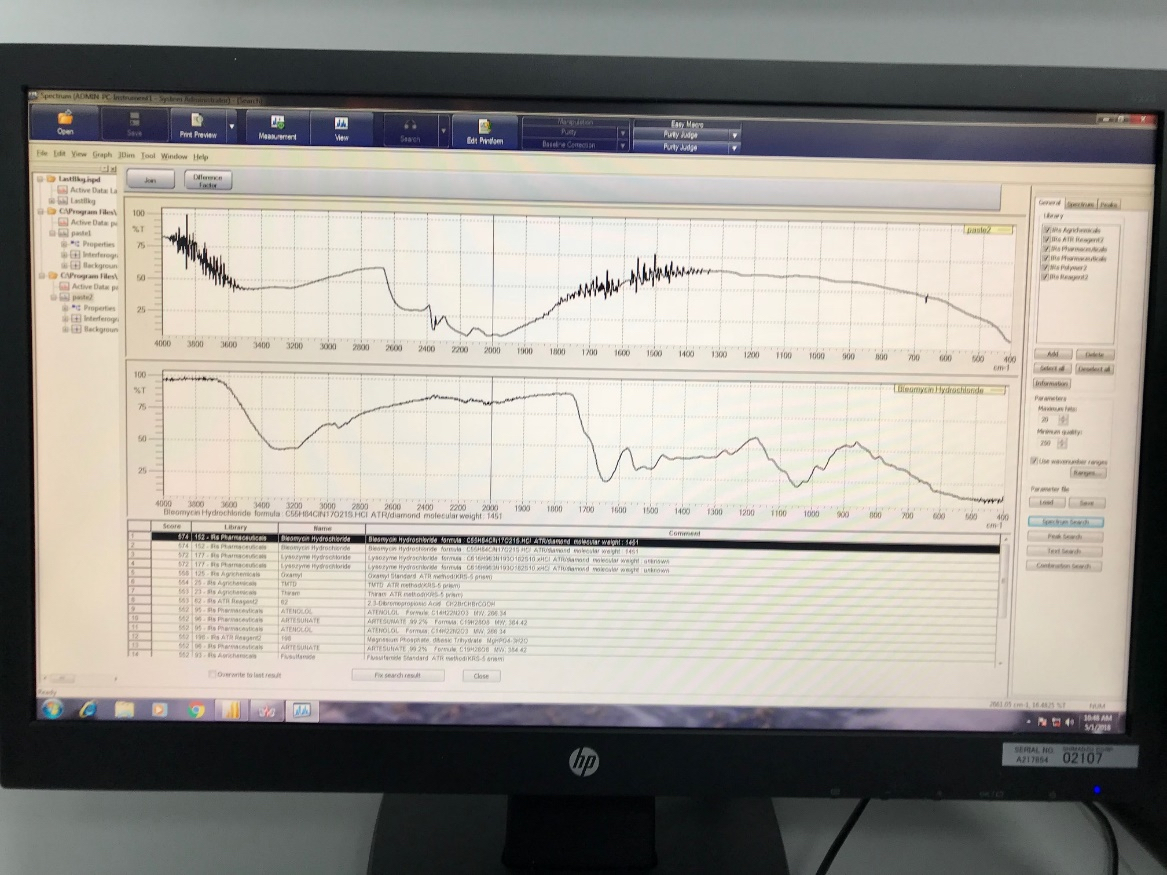
We will be using Fourier Transform InfraRed (FTIR) spectrometer with an Attenuated Total Reflectance (ATR) accessory (IRAffinity-1S by Shimadzu) which can provide us with accurate data that can be used to measure the degree of conversion. Additionally, samples will be taken from different types of RBCs with different resin matrices.
We will be measuring the uncured composite using the FTIR first and then we will be adjusting the LCU at different angles (90,60,45,30, degrees) while it’s fixed at a certain distance from the composite and take and run the test for each of them and then using a given mathematical formula, we can conclude the degree of conversion in a percentage, and this will be done for each type and brand of composite. In conclusion we can compare each angulation and its effect on the curing of the composite and to what degree it can alter the efficiency of light curing units.
Below are pictures showing the FTIR device that we will use in this study.
Effect of instructions on dentist’s ability to light-cure dental composites
Additionally, we have recently started a secondary study using the MARC Patient Simulator Which tests and measures the efficiency of the light curing, it is basically a phantom head with two sensors that collect the light from the LCUs and displays the data on a special software on a laptop connected to the head, it gives live data and stores it so we can compare between different tests statistically.
In this study a group of the internship trainees will be performing the tests, each one of them will do four tests, two before any instructions (one on a simulated anterior restoration and one posterior) and then two tests after we give them the instructions (also one anterior and one posterior).
This will allow us to compare and perceive the effect of such instructions on the efficiency of light-curing which is usually over-looked during daily practice, which will help us to educate dental care professionals on this issue, additionally, we can compare between light-curing anterior and posterior restorations because we expect the posteriors restorations to receive less efficient light-curing than anterior restorations, therefor we can further instruct the dentists and dental students on how to cure such restorations.